THE THORAX

Content -
• Thorax
• Areas of thorax
• Bones of thorax
• Muscle of thorax
• THE THORAX --
The thorax is the area of the body situated between the neck and the abdomen. The thorax itself can be split up into various areas that contain important structures.
The thorax is bound by bony structures including the 12 pairs of ribs and thoracic vertebrae, whilst also being supported by many ligaments and muscles.
The muscles of the thorax are also important for the vital actions of breathing and muscles that attach to the thoracic wall may also contribute to the general movement of the trunk, upper limbs and the neck.
The thoracic cavity is home to many vital organs, notably the lungs/pleurae and the heart, but also includes the thymus gland and the breasts. As the heart is found here, the great vessels associated with it are also found – including the pulmonary arteries/veins, the superior vena cava and the aorta (as well as some of its proximal branches).
In this section, learn more about the areas of the thorax, bones of the thorax, muscles of the thorax, organs of the thorax and the vasculature of the thorax.
AREAS OF THORAX -
In this section, learn more about the areas of the thorax– the superior mediastinum, the anterior mediastinum, the middle mediastinum and the posterior mediastinum.
The mediastinum is the area of the thorax located between the two pleural sacs and encloses most of the organs found in the thorax. The mediastinum can be split into the superior and inferior mediastinum. The inferior mediastinum itself can be further divided into the anterior, middle and posterior mediastinum, which all lie between the sternal angle and the diaphragm.
• superior mediastinum -
The superior mediastinum is the area of the thorax above the sternal angle (at the level of the T4 vertebra) and between the thoracic aperture. Some of the contents of the superior mediastinum include the arch of the aorta, the superior vena cava, the trachea and the vagus nerve.
• Anterior mediastinum -
The anterior mediastinum lies in front of the middle mediastinum and contains no major structures whereas the posterior mediastinum contains the thoracic aorta, oesophagus, thoracic duct, azygos system of veins, as well as the sympathetic trunks.
• Middle mediastinum -
The middle mediastinum sits behind the anterior mediastinum and in front of the posterior mediastinum. The middle mediastinum contains the heart as well as the origins of its great vessels. Furthermore, the trachea notably bifurcates in here to form the right and left main bronchi.
• the posterior mediastinum -
The posterior mediastinum contains a number of major organs, blood vessels and nerves.
_________________________________________
BONES OF THORAX ( THORACIC CAGE )
The thoracic cage (rib cage) is the skeleton of the thoracic wall. It is formed by the 12 thoracic vertebrae, 12 pairs of ribs and associated costal cartilages and the sternum.
The thoracic cage takes the form of a domed bird cage with the horizontal bars formed by ribs and costal cartilages. It is supported by the vertical sternum or breastbone (anteriorly) and the 12 thoracic vertebrae (posteriorly). The thoracic cage can also be described as an osteocartilaginous cage formed by the sternum, 12 pairs of ribs and costal cartilages, 12 thoracic vertebrae and the intervertebral (IV) discs interposed between them.
The thoracic cage, like skeletal tissue in most parts of the body, serves to support the thorax. It also has several functions, such as:
- protecticting vital thoracic and abdominal internal organs from external forces
- resisting the negative internal pressures generated by the elastic recoil of the lungs and respiration-induced movements
- providing attachment for and supporting the weight of the upper limbs
- providing the anchoring attachment (origin) of many of the muscles that move and maintain the position of the upper limbs relative to the trunk.
| Sternum | Manubrium: suprasternal and clavicular notches, articulates with the body, first two ribs, and clavicles Body: articulates with the costal cartilages of second to seventh ribs and the xiphoid process (xiphisternal joint) Xiphoid process: T10 level, inferior limit of the central part of the thorax |
| Thoracic Vertebrae | Twelve in total, containing a body, arch, and costal facets |
| Ribs | Typical: head, beck, tubercle, body Atypical: one or two facets and a tuberosity (1st, 2nd, 10th-12th) True: 1st to 7th, contain their own costal cartilages and attach directly to the sternum False: 8th, 9th, 10th of which their respective cartilages connect to the costal cartilage of the rib above Floating: 11th and 12th rib hang freely and only articulate with the vertebra |
| Intercostal Spaces | Named according to the rib forming the superior border and contain intercostal muscles, vessels, and nerves |
| Joints | Xiphisternal: xiphoid process and body of sternum Intervertebral: between vertebrae Sternochondral: sternum and costal cartilages Sternoclavicular: manubrium and clavicles Manubriosternal: manubrium and body of sternum Costochondral: costal cartilage and rib Costovertebral: formed by the ribs and bodies of the vertebrae. Interchondral: joining the costal cartilages to one another |
Ossification and development
During the intrauterine period of development, the rib cage begins to ossify. This process continues until approximately the 25th year of extra-uterine life. Of all the three groups of bones forming the thoracic cage, the vertebral and ribs ossification start by the end of the embryonic period (at approximately the 7th week of gestation). Sternal ossification begins during the 5th month of fetal development.
Although ossification is complete, on average, by age 25 years, progressive calcification of the costal cartilages can continue into old age. A notably significant development of the thoracic cage is the expansion of the rib cage which contributes greatly to the broad shoulders observed particularly in males. In males, expansion of the rib cage is caused by the effects of testosterone hormone during puberty; thus males generally have broad shoulders and expanded thoraces, allowing them to inhale more air to supply their muscles with oxygen.
Sternum
The sternum (derived from the Greek word, sternon meaning chest) is a flat, elongated bone forming the middle of the anterior part of the thoracic cage.
The sternum consists of three parts, namely, the manubrium, body of sternum and the xiphoid process.
Manubrium
The manubrium is a roughly trapezoidal bone. It is the widest and thickest of the three parts of the sternum. Its superior border has an easily palpated concave centre, called the jugular notch (or suprasternal notch). Lateral to the suprasternal notch are the clavicular notches, which receive the sternal end (medial end) of the clavicle. In an articulated skeleton, the jugular notch is deepened by the medial ends of the left and right clavicles.
The manubrium also articulates with the costal cartilage of the first rib – the synchondrosis of the first rib, as well as the superior half of the articular surface of the costal cartilage of the second rib.
The manubrium and body of the sternum lie in slightly different planes superiorly and inferiorly to their junction, the manubriosternal joint; hence, their junction forms a projecting sternal angle (of Louis).
Body
The body of the sternum is longer, narrower and thinner than the manubrium. It is interposed between the manubrium and the xiphoid process, and is located at the level of the T5 – T9 vertebrae. On the lateral borders, the body articulates with the costal cartilages of the second to seventh ribs, and forms a xiphisternal joint at its junction with the xiphoid process.
Xiphoid process
The xiphoid process is the smallest and most variable part of the sternum. It is thin, elongated and lies at the level of the T10 vertebra. Although often pointed in some individuals, the process may be blunt, bifid, curved or deflected to one side or anteriorly. The xiphoid process is small and cartilaginous in young people but gets ossified in adults older than age 40, with severe pains accompanying the process of ossification. Ossification of the xiphoid process in the elderly people may also cause fusion of the xiphoid process with the sternal body.
The xiphoid process is an important landmark in the median plane, indicating the inferior limit of the central part of the thoracic cavity. This inferior limit corresponds to the xiphisternal joint, and it is also the site of the infrasternal angle (subcostal angle) of the inferior thoracic aperture. Additionally, the xiphoid process is a midline marker for the superior limit of the liver, the central tendon of the diaphragm, and the inferior border of the heart.
Have you been wondering whether you should use 3D anatomy tools to learn about the thoracic cage? Here's why you should think again.
Thoracic vertebrae
The thoracic vertebrae are a group of 12 small bones that form the vertebral spine of the thorax. They are intermediate in size between those of the cervical region and lumbar region, to which they are also interposed, and increase in size from above downwards.
They are mostly typical vertebrae in that they are independent, have bodies, vertebral arches, and seven processes for muscular and articular connections. Most of them also have costal facets on their transverse processes for articulation with the tubercles of ribs. They are also characterized with bilateral costal facets (demifacets) on their bodies, and long, inferiorly slanting spinous processes.
Atypical thoracic vertebrae have “whole costal facets” in place of demifacets. The T1 vertebrae, T10, T11 and T12 are all atypical, having only single whole costal facets.
Learn the bones of the thoracic cavity with the following study unit:
:format(jpeg)/images/study_unit/anatomy-of-sternum/jJBSNkS35HGwZXgrAoZDrg_Sternum.png)
Ribs and costal cartilages
The ribs (derived from the Latin word costae) are curved, long bones connecting the sternum and most of the thoracic vertebrae (specifically T1-T10). They make up the highest number of bones forming the thoracic cage. They are remarkably light in weight yet highly resilient to pressure from within the thorax, e.g., pressure generated during inspiration.
There are three types of ribs, and all groups have a spongy interior containing bone marrow (hematopoietic tissue), which forms blood cells. All of the ribs that articulate (rib 1-10) with the sternum are prolonged anteriorly, with their attached costal cartilages with which they articulate with the sternum. These costal cartilages also contribute to the elasticity of the thoracic wall, providing a flexible attachment for their anterior or distal ends.
The cartilages of the first 8 ribs increase in length in descending order, with the length then decreasing after the 8th. The first seven (and sometimes the 8th) cartilages attach directly and independently to the sternum. The 8th, 9th and 10th cartilages articulate with the costal cartilages just superior to them, forming a continuous, articulated, cartilaginous costal margin of the rib cage. The ribs can be divided into two groups, typical and atypical.
Typical ribs
The typical ribs include ribs 3 to 9th and have the following components:
- Wedge shaped head with two facets, separated by the crest of the head.
- Neck connecting the head with the body at the level of the tubercle.
- A tubercle at the junction of the neck and body, which and has a smooth articular part for articulating with the transverse process of the corresponding vertebra.
- A thin, flat and curved body (shaft), most markedly at the costal angle where the rib turns anterolaterally.
Atypical ribs
The atypical ribs are the 1st, 2nd, and the 10th – 12th ribs characterized with the following features:
- Have one or two facets, and a rough area on the superior surface, e.g, the tuberosity for serratus anterior of the second rib.
True, false, floating ribs
All 12 pairs of ribs can also be divided into the following types or groups:
- True (Vertebrocostal) ribs: The 1st to 7th ribs fall under this group, and they attach directly to the sternum through their own costal cartilages.
- False (vertebrochondral) ribs: The 8th, 9th, and 10th ribs are referred to as false ribs because their cartilages are connected to the costal cartilage of the rib above them; thus their connection with the sternum is indirect.
- Floating (vertebral, free) ribs: The 11th and 12th ribs are grouped as floating ribs. They articulate only to the vertebral column, thus hanging freely. Some authors group the 10th rib with the floating ribs; and the rudimentary cartilages of these floating ribs do not connect even indirectly with the sternum, instead they end in the posterior abdominal musculature.
Intercostal spaces
Intercostal spaces are occupied by intercostal muscles and membranes, 11 intercostal nerves and two sets (main and collateral) of intercostal blood vessels also identified by the same number assigned to the intercostal space. Below the 12th rib, is referred to as the subcostal space and the anterior ramus of the spinal nerve T12 runs through this space, and it is thus referred to as the subcostal nerve.
Joints
The joints forming the domed-shaped thoracic cage include the:
- Xiphisternal joint – xiphoid process and body of sternum
- Intervertebral joints – between vertebrae
- Sternochondral joints – sternum and costal cartilages
- Sternoclavicular joints – manubrium and clavicles
- Manubriosternal joints – manubrium and body of sternum
- Costochondral joints – costal cartilage and rib
- Costovertebral joints – formed by the ribs and bodies of the vertebrae.
- Interchondral joints – joining the costal cartilages to one another.
Some of the above joints are briefly described below.
Costochondral joints
The costochondral joints are the articulations between each rib and its costal cartilage. It is a hyaline cartilaginous type of joint. The articulation is between the cup-shaped depression in the sternal end of a rib and the lateral end of a costal cartilage. The rib and its cartilage are firmly bound together by the continuity of the periosteum of the rib with the perichondrium of the cartilage. No movement normally occurs at these joints.
Interchondral joints
The interchondral joints are plane synovial joints between the adjacent borders of the 6th and 7th, 7th and 8th, and 8th and 9th costal cartilages. The joints are usually strengthened by interchondral ligaments, and they also have synovial cavities that are enclosed by joint capsules.
Sternocostal joints
These are joints formed by the lateral borders of the sternum and the costal cartilages of the 1st to 7th ribs, and sometimes the 8th rib. The first pair of costal cartilages articulate with the manubrium by means of a thin dense layer of tightly adherent fibrocartilage interposed between cartilage and the manubrium, the synchondrosis of the first rib. The second to seventh pairs of costal cartilages articulate with the sternum at synovial joints with fibrocartilaginous articular surfaces on both the chondral and sternal aspects, allowing movement during respiration. The sternocostal joints are also referred to as sternochondral joints.
Costovertebral joints
Articulation of the left and right ribs with the vertebral column (thoracic vertebrae) complete the domed birdcage-like thoracic cage posteriorly. The costovertebral joints are synovial joints, and they are richly surrounded by joint capsule. Of all the joints of the rib cage, these joints have the largest amount of ligaments crossing and stabilizing them.
Most of the ribs are attached firmly to the intervertebral (IV) discs by intra-articular ligament within the joints. Fanning around from the anterior margin of the heads of the ribs to the sides of the bodies of vertebrae and the IV discs between them is a radiate sternocostal ligament. Also crossing these joints is the costotransverse ligament passing from the neck of the rib to the transverse process, and a lateral costotransverse ligament passing from the tubercle of the rib to the tip of the transverse process. These ligaments strengthen the anterior and posterior aspects of the joints respectively. There is a superior costotransverse ligament which may be divided into a strong anterior costotransverse ligament and a weak posterior costotransverse ligament, both joining the crests of the neck of the ribs to the transverse processes superior to each of the ribs.
__&&&__________________________________
MUSCLE OF THORAX -
The diaphragm is a double-domed musculotendinous sheet, located at the inferior-most aspect of the rib cage. It serves two main functions:
- Separates the thoracic cavity from the abdominal cavity (the word diaphragm is derived from the Greek ‘diáphragma’, meaning partition).
- Undergoes contraction and relaxation, altering the volume of the thoracic cavity and the lungs, producing inspiration and expiration.
In this article, we shall look at the anatomy of the diaphragm – its attachments, actions and associated neurovascular structures.
Anatomical Position and Attachments
The diaphragm is located at the inferior-most aspect of the ribcage, filling the inferior thoracic aperture. It acts as the floor of the thoracic cavity and the roof of the abdominal cavity. The attachments of diaphragm can be divided into peripheral and central attachments. It has three peripheral attachments:
- Lumbar vertebrae and arcuate ligaments.
- Costal cartilages of ribs 7-10 (attach directly to ribs 11-12).
- Xiphoid process of the sternum.
The parts of the diaphragm that arise from the vertebrae are tendinous in structure, and are known as the right and left crura:
- Right crus – Arises from L1-L3 and their intervertebral discs. Some fibres from the right crus surround the oesophageal opening, acting as a physiological sphincter to prevent reflux of gastric contents into the oesophagus.
- Left crus – Arises from L1-L2 and their intervertebral discs.
The muscle fibres of the diaphragm combine to form a central tendon. This tendon ascends to fuse with the inferior surface of the fibrous pericardium. Either side of the pericardium, the diaphragm ascends to form left and right domes. At rest, the right dome lies slightly higher than the left – this is thought to be due to the presence of the liver.
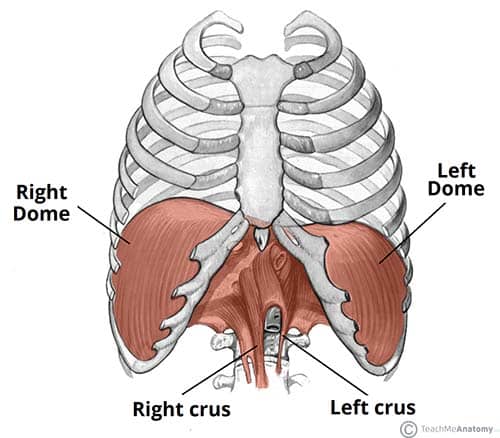
Fig 1.0 – The diaphragm is split into two lobes, left and right. Note the vertebral attachments of the diaphragm are the left and right crura.
Pathways through the Diaphragm
The diaphragm divides the thoracic and abdominal cavities. Thus, any structure that pass between the two cavities will pierce the diaphragm.

- Separates the thoracic cavity from the abdominal cavity (the word diaphragm is derived from the Greek ‘diáphragma’, meaning partition).
- Undergoes contraction and relaxation, altering the volume of the thoracic cavity and the lungs, producing inspiration and expiration.
In this article, we shall look at the anatomy of the diaphragm – its attachments, actions and associated neurovascular structures.
Anatomical Position and Attachments
The diaphragm is located at the inferior-most aspect of the ribcage, filling the inferior thoracic aperture. It acts as the floor of the thoracic cavity and the roof of the abdominal cavity. The attachments of diaphragm can be divided into peripheral and central attachments. It has three peripheral attachments:
- Lumbar vertebrae and arcuate ligaments.
- Costal cartilages of ribs 7-10 (attach directly to ribs 11-12).
- Xiphoid process of the sternum.
The parts of the diaphragm that arise from the vertebrae are tendinous in structure, and are known as the right and left crura:
- Right crus – Arises from L1-L3 and their intervertebral discs. Some fibres from the right crus surround the oesophageal opening, acting as a physiological sphincter to prevent reflux of gastric contents into the oesophagus.
- Left crus – Arises from L1-L2 and their intervertebral discs.
The muscle fibres of the diaphragm combine to form a central tendon. This tendon ascends to fuse with the inferior surface of the fibrous pericardium. Either side of the pericardium, the diaphragm ascends to form left and right domes. At rest, the right dome lies slightly higher than the left – this is thought to be due to the presence of the liver.
Fig 1.0 – The diaphragm is split into two lobes, left and right. Note the vertebral attachments of the diaphragm are the left and right crura.
Pathways through the Diaphragm
The diaphragm divides the thoracic and abdominal cavities. Thus, any structure that pass between the two cavities will pierce the diaphragm.
There are three openings that act as conduit for these structures:
| Caval Hiatus (T8) | Oesophageal Hiatus (T10) | Aortic Hiatus (T12) |
|
|
|
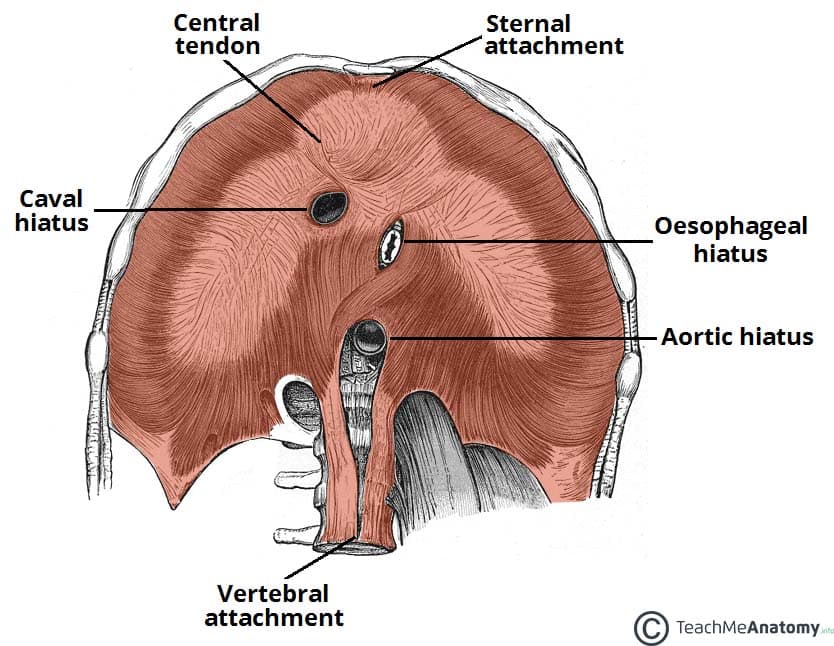
Fig 1.1 – View of the inferior surface of the diaphragm. Note the three openings.
Actions
The diaphragm is the primary muscle of respiration. During inspiration, it contracts and flattens, increasing the vertical diameter of the thoracic cavity. This produces lung expansion, and air is drawn in. During expiration, the diaphragm passively relaxes and returns to its original dome shape. This reduces the volume of the thoracic cavity.
Innervation and Vasculature
The halves of the diaphragm receive motor innervation from the phrenic nerve. The left half of the diaphragm (known as a hemidiaphragm) is innervated by the left phrenic nerve, and vice versa. Each phrenic nerve is formed in the neck within the cervical plexus and contains fibres from spinal roots C3-C5.
The majority of the arterial supply to the diaphragm is delivered via the inferior phrenic arteries, which arise directly from the abdominal aorta. The remaining supply is from the superior phrenic, pericardiacophrenic, and musculophrenic arteries. The draining veins follow the aforementioned arteries.
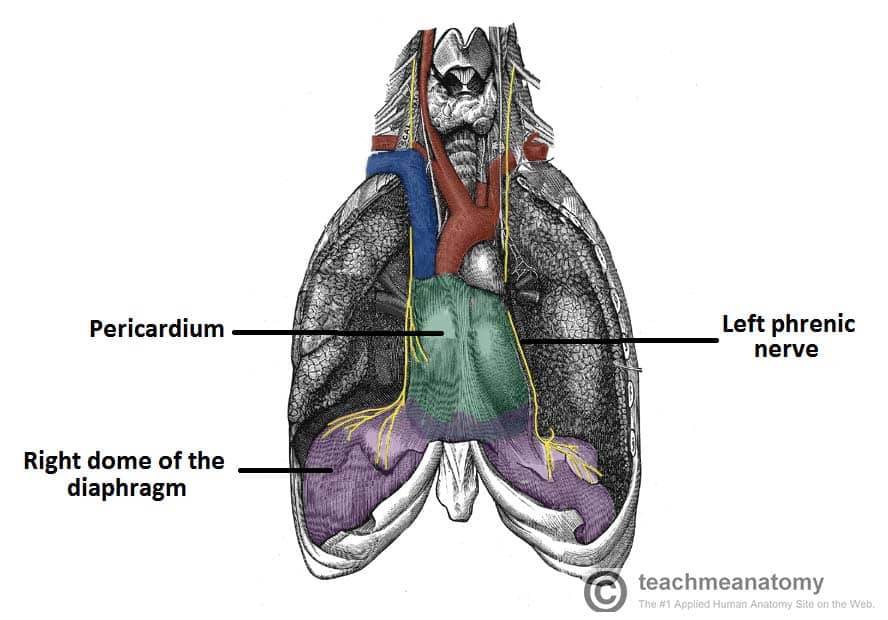
Fig 1.2 – The anatomical course of the phrenic nerves, which innervate the diaphragm.
Clinical Relevance: Paralysis of the Diaphragm
Diaphragmatic paralysis is due to an interruption in its nervous supply. This can occur in the phrenic nerve, cervical spinal cord, or the brainstem. It is most often due to a lesion of the phrenic nerve:
- Mechanical trauma: ligation or damage to the nerve during surgery.
- Compression: due to a tumour within the chest cavity.
- Myopathies: such as myasthenia gravis.
- Neuropathies: such diabetic neuropathy.
Paralysis of the diaphragm produces a paradoxical movement. The affected side of the diaphragm moves upwards during inspiration, and downwards during expiration. A unilateral diaphragmatic paralysis is usually asymptomatic and is most often an incidental finding on x-ray. If both sides are paralysed, the patient may experience poor exercise tolerance, orthopnoea and fatigue. Lung function tests will show a restrictive deficit.
Management of diaphragmatic paralysis is two-fold. Firstly, the underlying cause must be identified and treated. The second part of treatment deals with symptomatic relief. This is usually via non-invasive ventilation, such as a CPAP (continuous positive airway pressure) machine.
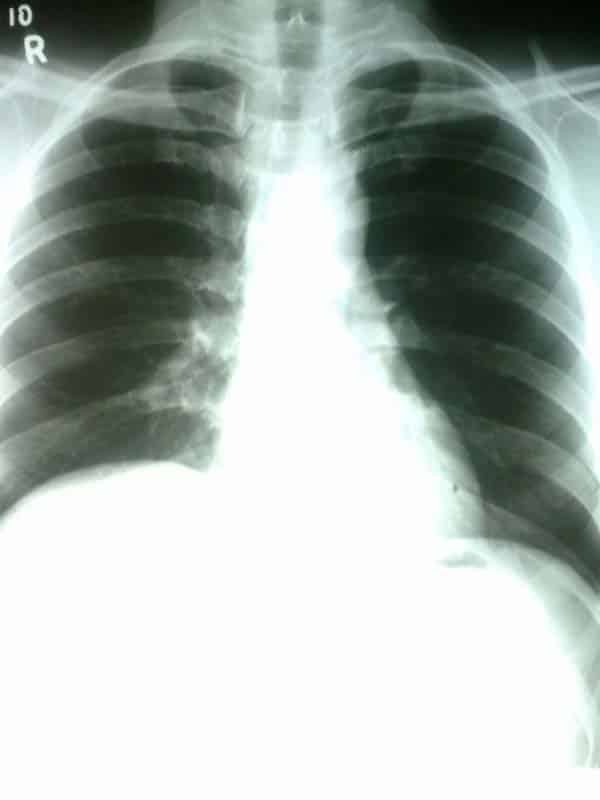
Fig 3 – Chest x-ray, showing paralysis of the right hemidiaphragm.
__________________________________________
The Muscles of the Thoracic Cage
There are five muscles that make up the thoracic cage; the intercostals (external, internal and innermost), subcostals, and transversus thoracis. These muscles act to change the volume of the thoracic cavity during respiration.
There are some other muscles that do not comprise the thoracic wall, but do attach to it. These include the pectoralis major, minor, serratus anterior and the scalene muscles.
Intercostals
The intercostal muscles lie in the intercostal spaces between ribs. They are organised into three layers.
External Intercostals
There are 11 pairs of external intercostal muscles. They run inferoanteriorly from the rib above to the rib below, and are continuous with the external oblique of the abdomen.
- Attachments: Originate at the lower border of the rib, inserting into the superior border of the rib below.
- Actions: Elevates the ribs, increasing the thoracic volume.
- Innervation: Intercostal nerves (T1-T11).
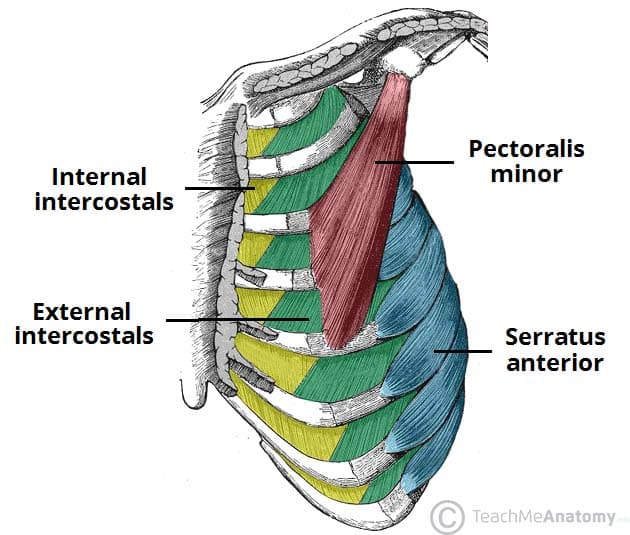
Fig 1 – The external and internal intercostals of the thoracic wall.
Internal Intercostals
These flat muscles lie deep to the external intercostals. Like the external intercostals, they run from the rib above to the one below, but in an opposite direction (inferoposteriorly). They are continuous with the internal oblique muscle of the abdominal wall.
- Attachments: Originates from the lateral edge of the costal groove and inserts into the superior surface of the rib below.
- Actions: The interosseous part reduces the thoracic volume by depressing the ribcage, and the interchondral part elevates the ribs.
- Innervation: Intercostal nerves (T1-T11).
Innermost Intercostals
These muscles are the deepest of the intercostal muscles, and are similar in structure to the internal intercostals.
They are separated from the internal intercostals by the intercostal neurovascular bundle and are found in the most lateral portion of the intercostal spaces.
- Attachments: Originates from the medial edge of the costal groove and inserts into the superior surface of the rib below.
- Actions: The interosseous part reduces the thoracic volume by depressing the ribcage, and the interchondral part elevates the ribs.
- Innervation: Intercostal nerves (T1-T11)
Transversus Thoracis
These muscles of the thoracic cage are continuous with transversus abdominis inferiorly.
- Attachments: From the posterior surface of the inferior sternum to the internal surface of costal cartilages 2-6.
- Actions: Weakly depress the ribs.
- Innervation: Intercostal nerves (T2-T6).
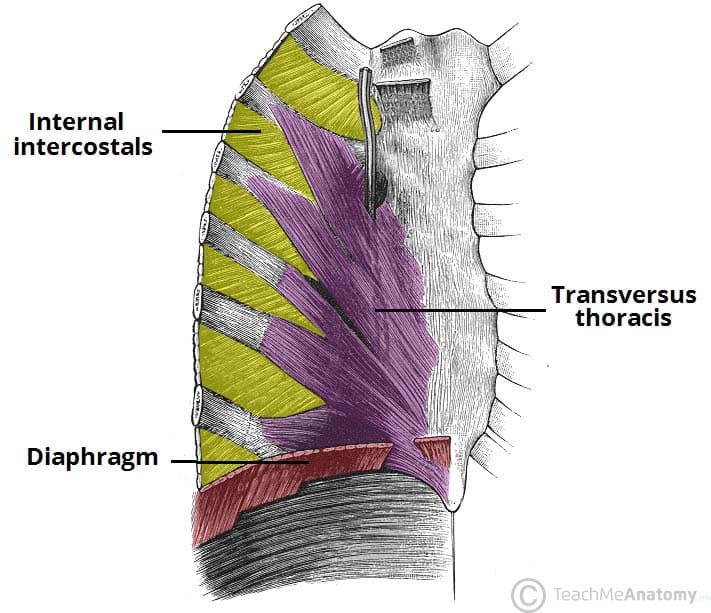
Fig 2 – View of the internal aspect of the thoracic wall. The internal intercostal and transverse thoracis muscles are visible.
Subcostals
The subcostal muscles are found in the inferior portion of the thoracic wall. They comprise of thin slips of muscle, which run from the internal surface of one rib, to second and third ribs below. The direction of the fibres parallels that of the innermost intercostal.
- Attachments: These originate from the inferior surface of the lower ribs, near the angle of the rib. They then attach to the superior border of the rib 2 or 3 below.
- Actions: Share the action of the internal intercostals
- Innervation: Intercostal nerves


Comments
Post a Comment